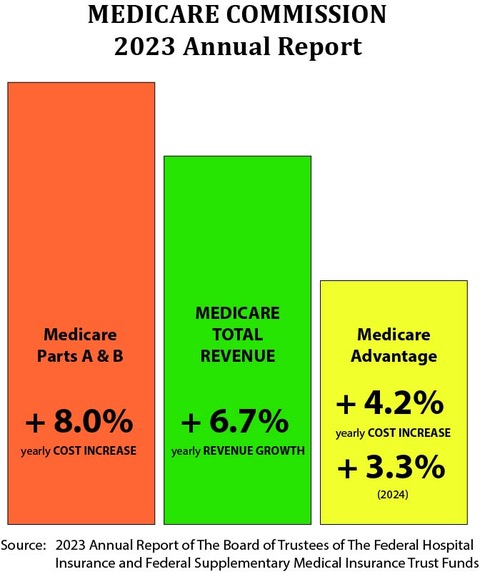
The graphic above shows the overall picture. (Source: Institute for InterGroup Understanding)
Here is one example:
The Medicare Advantage plans know that 90 percent of the amputations are caused by foot ulcers and that you can reduce foot ulcers by over 40 percent with clean socks and dry feet. Medicare Advantage plans have staff working on dry feet and clean socks, [while] the fee-for-service providers who make more than $100,000 for each amputation in their fees actually had an increase in cases during covid because it’s so profitable.
The [MA] special-needs plans had almost no amputations.
The information here is well-intended, and the MA special-needs plans do have an excellent record.
But this post contains a snide comments about “fee for service providers.”
Consider the following from a 2009 article:
“According to an article from HealthLeaders Media, the American College of Surgeons noted in a statement that Medicare actually reimburses surgeons between $740 and $1,140 for a leg amputation — and private insurers tend to have similar rates. But Obama’s numbers were not made up: According to the Journal of the American Podiatric Medical Association, a foot or leg amputation costs between $30,000 and $60,000 in initial hospital costs, plus between $43,000 and $60,000 in costs for follow-up care over the next three years. So even though individual doctors may not have a large financial incentive to perform them, amputations are costly to the health insurance system.”
In other words, the surgeons are not making the big bucks here. See any interviews with Dr Kevin Smith for more examples.
“In other words, the surgeons are not making the big bucks here.”
Well Bob, here’s a 2020 article in which you’ll find median physician incomes by specialty; scroll down to the appropriate table:
//physiciansthrive.com/wp-content/uploads/2020/11/Compensation-Report-2020.pdf
(You may need to prefix an https:)
The table shows that, when the term “surgeons” is disaggregated, the very highest median incomes for all physicians are surgeons- orthopedic, cardiovascular, and neurosurgeons. Their median annual incomes range between $500,000 and $645,000. They may not make it on their Medicare patients but they are making it.
From my perch $500,000 + per year is “big bucks”.
It’s no big secret that Medicare reimburses lesser amounts for non-hospital covered Medicare expenses than private insurers do for the same expenses incurred by the non-Medicare population. In fact, skimpy Medicare reimbursements have repeatedly been identified as the reason for so-called “cost-shift” from Medicare patients to privately- insured patients – but that’s a discussion for another day.
Anyway, the question you raise is not simply whether hospitals charge more for surgery than the surgeon does. Of course they do. But, according According to AHA more than 30% of hospitals had negative margins in 2019. The COVID years did not help their financial performance. Perhaps hospitals do not charge enough? Meanwhile surgeons are doing quite well.
‘tis a puzzlement.” Yes?
There are some neat interviews with Dr Keith Smith. He founded the Surgery Center of Oklahoma because he and fellow surgeons were angry at how little they got paid vs. the hospitals where surgery took place.
These interviews are 5-10 years old though. Changes may have happened.
I suspect that surgeons put up with low Medicare payments because they are so well paid by under-65 insurers.
Private insurers aren’t paying “big bucks” to any physicians out of the kindness of their hearts. They pay according to their contracts. Or, if instead insurers reimbursed all physician services at Medicare rates, insurers’ costs would be less than they are now, meaning their premiums would be less, meaning they would be more competitive. But wouldn’t at least one insurer already have thought of that?
And just imagine how the incomes of highest-paid physicians would change if Medicare reimbursement rules extended to all patients, not just those under age 65.
In that case, no payer would reimburse physicians for Medicare-related expenses that current Medicare reimbursement rates don’t cover. Docs won’t like that one bit. But it would happen with Bernie’s Medicare for All scheme for example, or anyone else’s idea for national medical insurance. And economists know (even though some won’t admit it) price controls cause more problems than they solve.
Well Bob this has been another interesting excursion but after all does not change the conclusion presented above by John Goodman. The evidence shows Medicare Advantage insurers are doing a better job of managing their costs than Medicare.